

Background:
HR-SMM is a plasma cell disorder with a 5-year risk of progression to symptomatic multiple myeloma (MM) of ~75% without therapy. Early treatment with novel therapies, may decrease the risk of progression and prolong survival as evidenced by studies (Quiredex and ECOG E3A06) comparing lenalidomide ± dexamethasone to observation. Randomized studies in MM have demonstrated that triplet are superior to doublet regimens and whole exome sequencing in HR-SMM suggests a more treatment-sensitive biology. Together, these support our initial pilot study (Korde et al, JAMA Onc 2015) in using effective therapy with KRd-R as early intervention. Given the favorable initial results of our pilot in terms of minimal residual disease (MRD) negativity rates, we designed a single-arm, phase 2 study with the primary objective of determining the rate of MRD negative complete remissions. Herein, we show that rates of MRD negativity are high and they are sustained with the use of KRd-R.
Methods:
Patients with HR-SMM (Mayo Clinic or PETHEMA models) received eight 28-day cycles of carfilzomib 20/36 mg/m2 IV days 1, 2, 8, 9, 15, 16; lenalidomide 25 mg PO days 1-21, and dexamethasone 20/10 mg days 1, 2, 8, 9, 15, 16, 22, 23. Transplant eligible patients underwent stem cell collection after 4 cycles of KRd and then resumed treatment without an intent for early high-dose melphalan with stem cell support (HDM-ASCT). After 8 cycles of KRd, patients transitioned to receive maintenance therapy with lenalidomide 10 mg PO days 1-21 for 24 additional cycles. Prophylactic antiviral and anticoagulation was mandated for all. MM laboratory evaluations were performed at the start of every cycle during KRd and every 3 cycles during -R and every 3 months during indefinite follow up. Bone marrow biopsies and PET/CTs were performed by the end of cycle 8 induction and then annually indefinitely. The primary objective was to determine the rate of MRD negative remissions by validated multi-color flow cytometry (≤10-5 sensitivity). Key secondary objectives included progression free survival (PFS) to symptomatic myeloma and biochemical progression per IMWG, duration of MRD negativity, overall response rate (ORR), and duration of response.
Results:
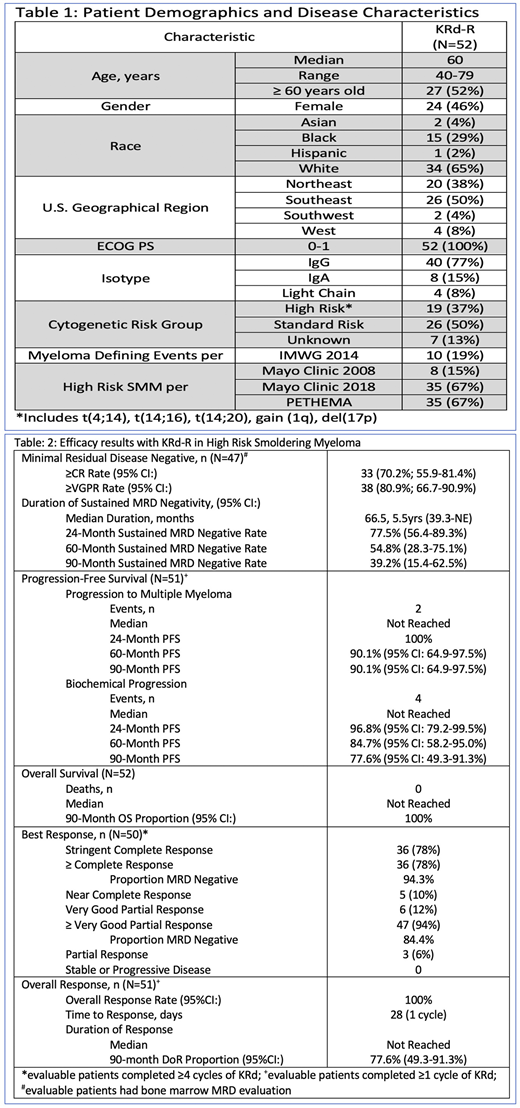
As of 7/15/2020, 52 patients meeting eligibility criteria were enrolled and their demographics and disease characteristics are shown in Table 1. With a median potential follow up of 27.3 months, the primary objective of MRD negative CR rate was 70.2% and the MRD negative ≥VGPR rate was 80.9%, Table 2. The median duration of MRD negativity was 5.5 years with 2 and 5 -year rates of 78% and 55%, respectively. The median time to progression to MM and time to biochemical progression was not reached with 90-month rates of 90% and 78%, respectively - 2 patients progressed to symptomatic MM and 4 patients biochemically. The ORR was 100% and 78% achieved a best response of stringent CR. No deaths occurred. All grade and Grade 3-4 treatment-related adverse events occurred in 90% and 33% of patients, respectively. Grade 3-4 toxicities occurring in >1 patient included neutropenia (19%), lymphopenia (13%), thromboembolism (12%), anemia (8%), rash (8%), leukopenia (6%), lung infection (6%), ALT increase (4%), diarrhea (4%), hyperglycemia (4%), hypophosphatemia (4%), and thrombocytopenia (4%). Other Grade 3-4 adverse events of interest occurring in ≤1 patient included atrial fibrillation, creatinine increase, dyspnea, febrile neutropenia, heart failure, hypertension, and neoplasm. Treatment discontinuation occurred in 4 patients; 3 due to toxicity and 1 due to patient withdrawal.
Conclusions:
Treatment of HR-SMM with KRd-R to prevent symptomatic MM resulted in an MRD negative CR rate of 70% with a median duration of 5.5 years. At the 5-year landmark, only 10% of patients developed MM which is favorable compared to historical rates with no treatment of ~75%. Alternative approaches using monotherapy lenalidomide (Lonial et al, JCO 2019) resulted in no CRs and a 5-year progression rate of 22% with a treatment discontinuation rate of 51% compared to 7% in our study. More aggressive approaches include GEM-CESAR (Mateos et al, ASH 2019) incorporating HDM-ASCT with KRd-R. Importantly, the rate of MRD negativity reported in GEM-CESAR was 56% compared to 70% in this study. Overall, the benefit compared to risk with KRd in SMM is very favorable. Future randomized trials will be needed to lock in this conclusion.
Korde:Amgen: Research Funding; Astra Zeneca: Other: Advisory Board. Mailankody:Physician Education Resource: Honoraria; PleXus Communications: Honoraria; Takeda Oncology: Research Funding; Janssen Oncology: Research Funding; Allogene Therapeutics: Research Funding; Juno Therapeutics, a Bristol-Myers Squibb Company: Research Funding. Manasanch:Quest Diagnostics: Research Funding; Sanofi: Research Funding; JW Pharma: Research Funding; Merck: Research Funding; Takeda: Honoraria; GSK: Honoraria; Sanofi: Honoraria; BMS: Honoraria; Adaptive Biotechnologies: Honoraria; Novartis: Research Funding. Bhutani:BMS: Other: Clinical trial funding to institute, Speakers Bureau; Amgen: Speakers Bureau; MedImmune: Other: Clinical Trial Funding to Institute; Janssen: Other: Clinical Trial Funding to Institute; Prothena: Other: Clinical Trial Funding to Institute; Sanofi Genzyme: Consultancy; Takeda: Other: Clinical trial funding to institute, Speakers Bureau. Landgren:Amgen: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria; Merck: Other; Karyopharma: Research Funding; Merck: Other; Pfizer: Consultancy, Honoraria; Juno: Consultancy, Honoraria; Cellectis: Consultancy, Honoraria; Glenmark: Consultancy, Honoraria, Research Funding; Seattle Genetics: Research Funding; Juno: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Karyopharma: Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Glenmark: Consultancy, Honoraria, Research Funding; Takeda: Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Janssen: Consultancy, Honoraria, Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Binding Site: Consultancy, Honoraria; Takeda: Other: Independent Data Monitoring Committees for clinical trials, Research Funding; BMS: Consultancy, Honoraria; Cellectis: Consultancy, Honoraria; BMS: Consultancy, Honoraria; Binding Site: Consultancy, Honoraria; Adaptive: Consultancy, Honoraria; Seattle Genetics: Research Funding.
carfilzomib, lenalidomide, and dexamethasone are not approved for smoldering myeloma.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal